Breast Reconstruction Surgery is the surgical process of rebuilding the shape and look of a breast, most commonly in women who have had surgery to treat breast cancer. It involves using autologous tissue, prosthetic implants, or a combination of both with the goal of reconstructing a natural-looking breast. This process often also includes the rebuilding of the nipple and areola, known as nipple-areola complex (NAC) reconstruction, as one of the final stages.
Generally, the aesthetic appearance is acceptable to the woman, but the reconstructed area is commonly completely numb afterwards, which results in loss of sexual function as well as the ability to perceive pain caused by burns and other injuries.
Timing
Breast reconstruction can be performed either immediately following the mastectomy or as a separate procedure at a later date, known as immediate reconstruction and delayed reconstruction, respectively. The decision of when breast reconstruction will take place is patient-specific and based on many different factors. Breast reconstruction is a large undertaking that usually requires multiple operations. These subsequent surgeries may be spread out over weeks or months.
Immediate Reconstruction
Breast reconstruction is termed "immediate" when it takes place during the same procedure as the mastectomy. Within the United States, approximately 35% of women who have undergone a total mastectomy for breast cancer will choose to pursue immediate breast reconstruction. One of the inherent advantages of immediate reconstruction is the potential for a single-stage procedure. This also means that the cost of immediate reconstruction is often far less to the patient. It can also reduce hospital costs by having fewer procedures and requiring a shorter length of the stay as an inpatient. Additionally, immediate reconstruction often has a better cosmetic result because of the preservation of anatomic landmarks and skin. With regards to psychosocial outcomes, opinions on timing have shifted in favor of immediate reconstruction. Originally, delayed reconstruction was believed to provide patients with time to psychologically adjust to the mastectomy and its effects on body image. However, this opinion is no longer widely held. Compared to delayed procedures, immediate reconstruction can have a more positive psychological impact on patients and their self-esteem, most likely due to the post-operative breast more closely resembling the natural breast compared to the defect left by mastectomy alone.
Delayed Reconstruction
Delayed breast reconstruction is considered more challenging than immediate reconstruction. Frequently not just breast volume, but also skin surface area needs to be restored. Many patients undergoing delayed breast reconstruction have been previously treated with radiation or have had a reconstruction failure with immediate breast reconstruction. In nearly all cases of delayed breast reconstruction tissue must be borrowed from another part of the body to make the new breast. Patients expected to receive radiation therapy as part of their adjuvant treatment are also commonly considered for delayed autologous reconstruction due to significantly higher complication rates with tissue expander-implant techniques in those patients. While waiting to begin breast reconstruction until several months after radiation therapy may decrease the risk of complications, this risk will always be higher in patients who have received radiation therapy. As with many other surgeries, patients with significant medical comorbidities (e.g., high blood pressure, obesity, diabetes) and smokers are higher-risk candidates. Surgeons may choose to perform delayed reconstruction to decrease this risk.
Techniques
There are several techniques for breast reconstruction. These options are broadly categorized into two different groups:
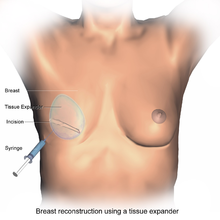
Breast reconstruction using a tissue expander, which is later replaced by a permanent prosthetic implant.
Implant-Based Reconstruction
This is the most common technique used worldwide. Implant-based reconstruction is an option for patients who have sufficient skin after mastectomy to cover a prosthetic implant and allow for a natural shape. For women undergoing bilateral mastectomies, implants provide the greatest opportunity for symmetrical shape and lift. Additionally, these procedures are generally much faster than flap-based reconstruction since tissue does not have to be taken from another part of the patient's body.
Typically, at the time of the mastectomy, the surgeon will insert a tissue expander underneath the pectoralis major muscle of the chest wall. This temporary silastic implant is used to hold tension on the mastectomy flaps. In doing so, the tissue expander prevents the breast tissue from contracting and allows for use of a larger implant later on compared to what would be safe at the time of the mastectomy. Following this initial procedure, the patient must return to the clinic on multiple occasions for saline to be injected into a tube inside the tissue expander. By doing this slowly over the course of several weeks, the space beneath the pectoralis major muscle is safely expanded to an appropriate size without causing too much stress on the breast tissue. A second procedure is then necessary to remove the tissue expander and replace it with the final, permanent prosthetic implant.

A permanent prosthetic implant eventually replaces the tissue expander.
Although in the past, prosthetic implants were placed directly under the skin, this method has fallen out of favor because of the greater risk of complications, including visible rippling of the implant and capsular contracture. The sub-pectoral technique described above is now preferred because it provides an additional muscular layer between the skin and the implant, decreasing the risk of visible deformity. Oftentimes, however, the pectoralis major muscle is not sufficiently large enough to cover the inferior portion of the prosthetic implant. If this is the case, one option is to use an acellular dermal matrix to cover the exposed portion of the prosthetic implant, improving both functional and aesthetic outcomes. This prepectoral space has recently, however, come back into practice. Both delayed and direct-to-implant reconstruction in this plane has been shown to be favourable.
Of note, a Cochrane review published in 2016 concluded that implants for use in breast reconstructive surgery have not been adequately studied in good quality clinical trials. "These days - even after a few million women have had breasts reconstructed – surgeons cannot inform women about the risks and complications of different implant-based breast reconstructive options on the basis of results derived from Randomized Controlled Trials."
Flap-Based Reconstruction
Flap-based reconstruction uses tissue from other parts of the patient's body (i.e., autologous tissue) such as the back, buttocks, thigh or abdomen. In surgery, a "flap" is any type of tissue that is lifted from a donor site and moved to a recipient site using its own blood supply. Usually, the blood supply is a named vessel. Flap-based reconstruction may be performed either by leaving the donor tissue connected to the original site (also known as a pedicle flap) to retain its blood supply (where the vessels are tunneled beneath the skin surface to the new site) or by cutting the donor tissue's vessels and surgically reconnecting them to a new blood supply at the recipient site (also known as a free flap or free tissue transfer). The latissimus dorsi is a prime example of such a flap since it can remain attached to its primary blood source which preserves the skins functioning, and is associated with better outcomes in comparison to other muscle and skin donor sites.

Transverse Rectus Abdominis Myocutaneous flap (TRAM).
One option for breast reconstruction involves using the latissimus dorsi muscle as the donor tissue. As a back muscle, the latissimus dorsi is large and flat and can be used without significant loss of function. It can be moved into the breast defect while still attached to its blood supply under the arm pit (axilla). A latissimus flap is often used to recruit soft-tissue coverage over an underlying implant; however, if the latissimus flap can provide enough volume, then occasionally it is used to reconstruct small breasts without the need for an implant. The latissimus dorsi flap has a number of advantages, but despite the advances in surgical techniques, it has remained vulnerable to skin dehiscence or necrosis at the donor site (on the back). The Mannu flap is a form of latissimus dorsi flap which avoids this complication by preserving a generous subcutaneous fat layer at the donor site and has been shown to be a safe, simple and effective way of avoiding wound dehiscence at the donor site after extended latissimus dorsi flap reconstruction.

Post-operative state after Transverse Rectus Abdominis Myocutaneous flap(TRAM).
Another possible donor site for breast reconstruction is the abdomen. The TRAM (transverse rectus abdominis myocutaneous) flap or its technically distinct variants of microvascular "perforator flaps" like the DIEP/SIEA flaps are all commonly used. In a TRAM procedure, a portion of the abdominal tissue, which includes skin, subcutaneous fat, minor muscles, and connective tissues, is taken from the patient's abdomen and transplanted to the breast site. Both TRAM and DIEP/SIEA use the abdominal tissue between the umbilicus (or "belly button") and the pubis. The DIEP flap and free-TRAM flap require advanced microsurgical technique and are less common as a result. Both can provide enough tissue to reconstruct large breasts and are a good option for patients who would prefer to maintain their pre-operative breast volume. These procedures are preferred by some breast cancer patients because removal of the donor site tissue results in an abdominoplasty (tummy tuck) and allow the breast to be reconstructed with one's own tissues instead of a prosthetic implant that uses foreign material. That said, TRAM flap procedures can potentially weaken the abdominal wall and torso strength, but they are generally well tolerated by most patients. Perforator techniques such as the DIEP (deep inferior epigastric perforator) flap and SIEA (superficial inferior epigastric artery) flap require precise dissection of small perforating vessels through the rectus muscle and, thus, do not require removal of abdominal muscle. Because of this, these flaps have the advantage of maintaining the majority of abdominal wall strength.
Other donor sites for autologous breast reconstruction include the buttocks, which provides tissue for the SGAP and IGAP (superior and inferior gluteal artery perforator, respectively) flaps. The purpose of perforator flaps (DIEP, SIEA, SGAP, IGAP) is to provide sufficient skin and fat for an aesthetic reconstruction while minimizing post-operative complications from harvesting the underlying muscles. DIEP reconstruction generally produces the best outcome for most women.
Mold-assisted reconstruction is a potential adjunctive process to help in flap-based reconstruction. By using a laser and 3D printer, a patient-specific silicone mold can be used as an aid during surgery, used as a guide for orienting and shaping the flap to improve accuracy and symmetry
After your surgery
You’re likely to feel tired and sore for a few days following your surgery, but you’ll be up and around in 24 to 48 hours. Most of your discomfort can be controlled by medication prescribed by your doctor. Within several days, the gauze dressings will be removed if you have them, and you will continue to wear the surgical bra for four weeks after your surgery. You may also experience a burning sensation in your nipples for about two weeks, but this will subside as bruising fades. Your stitches will come out in a week to 10 days, but the swelling in your breasts may take three to five weeks to disappear.